Since my first year of medical school, I have had an interest in wilderness medicine. What drew me in wasn’t just the adventure, it was the opportunity to learn the skills and knowledge to be the person others could rely on for medical care in a remote environment.
I have come to learn the importance of these skills. Whether it has been recreating in the backcountry, volunteering with search and rescue (SAR), or working as a wildland firefighter in my home province of British Columbia, I’ve faced situations in these settings that have taught me that providing care in the wilderness is vastly different from the hospital. But despite this, I had never formally trained in wilderness medicine.
In part, I don’t think it was a lack of interest, but rather a lack of access. For instance, as a Canadian medical student, there are no fourth-year wilderness medicine electives available at any of the medical schools in Canada, and there is limited exposure to wilderness medicine in preclinical teaching. So, in my final year, I looked internationally and found the Wilderness and Austere Medicine Elective at the University of New Mexico, an elective for medical students and residents that seemed to offer exactly what I had been searching for.
Fifteen of us arrived in New Mexico and were quickly immersed in our new environment. Within days, we were splitting time between classroom sessions at the UNM International Mountain Medicine Center and camping in the New Mexican high desert, learning core principles of wilderness care, survival, and land navigation. Early on, one concept stood out, the “Rule of Threes.”
At first, we learned it in the traditional survival sense. Our instructors asked us to think about what could kill us in three minutes, three hours, three days, three weeks, and three months in wilderness settings, and we brainstormed how to address each of these. By the end of this session, I found myself reflecting on how commonly some SAR subjects who are lost or stranded may prioritize finding food over addressing more immediate threats like warmth and shelter despite the latter being more imminent. Over the course of the following days, the Rule of Threes also evolved into something else: always having multiple ways to solve a problem. Three ways to purify water, build shelter, or manage a clinical scenario when your first plan fails.
I found myself applying this framework constantly, not just to survival skills, but to clinical thinking. What is my backup if this airway plan fails? What if I do not have the equipment I expect? What if I am alone?
That mindset extended into how I approached my medical kit. Before the course, I carried gear based largely on habit. During the elective, we were pushed to justify every item, how likely it is to be used, how much it weighs, and whether it can be improvised. Could one item serve multiple purposes instead of carrying several?
One example that stuck with me was the discussion around tourniquets. In wilderness settings, massive hemorrhage is time-sensitive and critical. While improvised solutions exist, they are unreliable. A commercial tourniquet, lightweight and compact, became an obvious addition to my kit. In addition, items like ski straps, which I had always carried for splitboarding, proved even more versatile than I expected, repeatedly used for splinting, securing gear, and patient packaging.
Week 1: Sand, Survival, & Scenarios

Left: Improvised splinting using ski straps for a patient with a simulated lower leg fracture during a scenario
Center (top): The International Mountain Medicine Center located on the UNM campus
Center (bottom): Starting a fire with a ferro rod and multitool
Right (top): Our basecamp for the land navigation and survival portion of the course
Right (bottom): Locating a subject using coordinates, map, and compass during a scenario
By the second week, we shifted into true mountain medicine and travelled to 10,800 ft in the Sangre de Cristo Mountains for a four-day yurt-based expedition. Here we practiced winter survival and learned to manage altitude illness, hypothermia, frostbite, and avalanche victims through lectures and daily scenarios.
Faculty encouraged us to try winter survival with the warmth of the yurt as a contingency nearby. On our first night, I dug a small snow cave and spent the night inside. Prior to this elective, I had considered this as a potential option in an emergency but was unsure whether it would actually be viable for an overnight shelter. To my surprise, while winds battered exposed tents, I was warm and sheltered. It reinforced that snow can be an effective insulating medium and that a small cave or trench can be built quickly and provide a reliable overnight shelter. After this, I feel more inclined to reach for my bivy sack over a tent on certain overnight trips needed for approaches.
Avalanche scenarios were some of the most high-yield learning for me. As a splitboarder, I had taken Avalanche Skills Training Level 1 and 2, which emphasize safety practices, decision making, and companion rescue. However, this course went further, teaching us victim triage and medical management.
The AvaLife Framework gave structure to something I had always found intimidating: multi-burial incidents. We were taught to triage based on burial depth and duration, allocating resources and directing resuscitation where survival was most likely. It transformed what felt chaotic into something systematic. I highly recommend checking out the AvaLife algorithms, which can be downloaded for free here and viewing the Union of International Mountain Leader Associations webinar here explaining the framework.
During our final scenario, I was assigned the role of Incident Commander. This was a shift outside my comfort zone. In many clinical environments, I am still heavily involved in hands-on care and focused on my individual tasks, but here I had to step back and lead.
We established roles using an Incident Command Structure, assigned teams, and outlined the resources we would need at our simulated field clinic. As the scenario unfolded, I watched the team execute, conducting a companion rescue, triaging patients, and initiating care. One patient had a massive lower extremity hemorrhage and a tension pneumothorax, another had fatal injuries, and a third had mild hypothermia and emotional distress.
With updates from the scene leader, I saw the medical team move quickly and effectively, addressing life threats while maintaining scene safety and delegating appropriately. At the same time, the rescue team packaged the critical patient in a hypothermia wrap and sked for evacuation.
What stood out most was not just the technical execution, but the coordination. Early in the course, scenarios had felt somewhat chaotic. By this point, we were functioning as a team, allowing me to focus on higher-level strategic priorities such as coordinating care and requesting resources.
Week 2: Alpine, Altitude, & Avalanche Victim Management
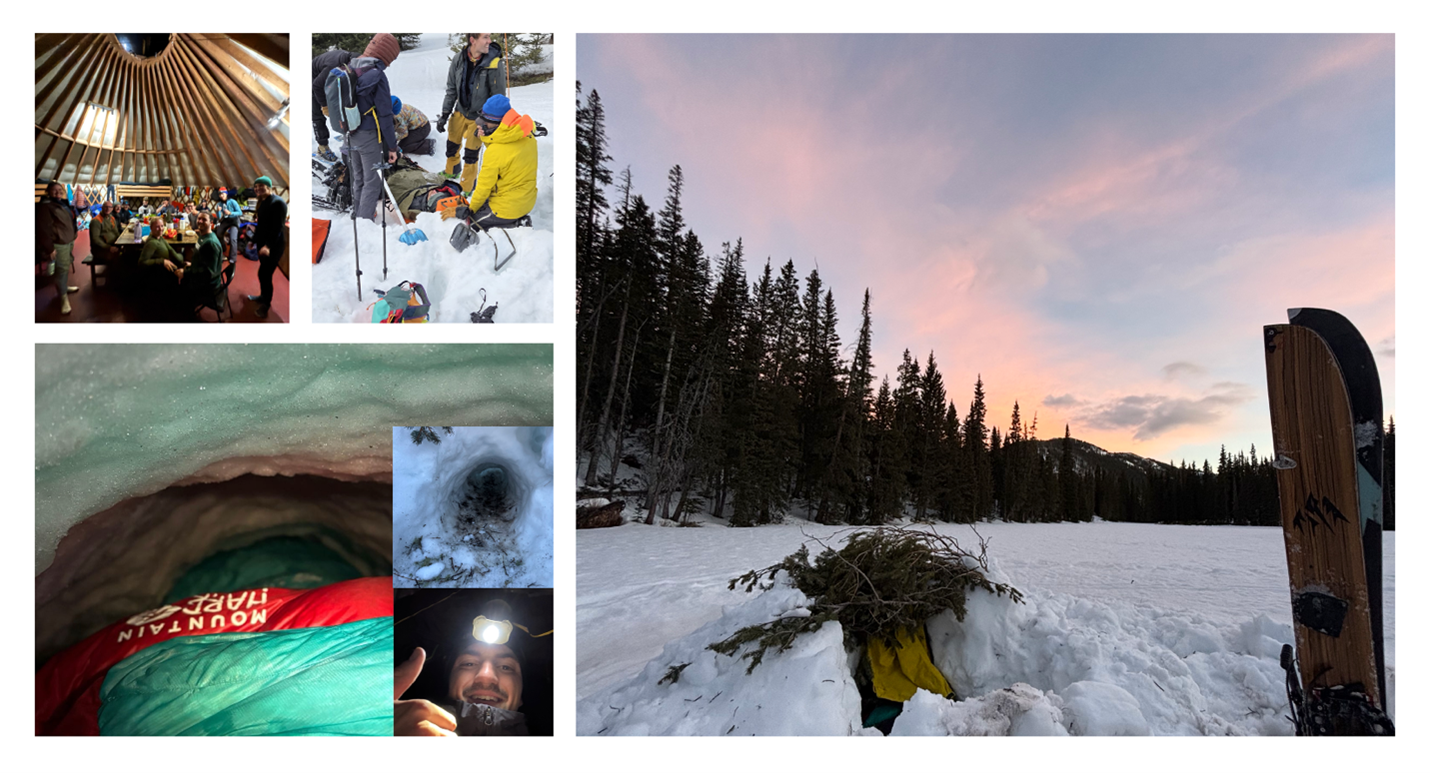
Left (top left): Our class having dinner in Bull of the Woods Yurt
Left (top right): Packaging a patient in a hypothermia wrap and sked for evacuation during an avalanche burial scenario
Bottom Left and Right: Sleeping in a snow cave
The third week brought us back to the classroom and into new environments. We covered topics ranging from exercise-associated hyponatremia to swiftwater rescue and spent time at local crags building hauling systems and refining rope skills. Again, I thought about the Rule of Threes: having multiple ways to build an anchor, rappel, or construct a mechanical advantage system for different scenarios.
We then transitioned onto the Colorado River for a multi-day rafting trip for our final week. What began as controlled practice on flatwater progressed into navigating Class III and IV rapids. In the evenings at camp, students gave mini-lectures, and we practiced technical skills such as knot tying and deploying throw bags.
Week 3 & 4: Rocks, Rope Rescue, & Rivers

Left (top): Hiking at Rattlesnake Canyon to stretch our legs during our trip down the Colorado River
Left (bottom): Paddling through a section of Vishnu Schist (black rock), which dates back about 1.7 billion years
Center: An evening lecture on river safety and trip logistics prior to our departure
Right: Practicing lowering and hauling rescuers at a local crag in Albuquerque as part of the rope rescue portion of the course
Looking back, what surprised me most about this elective was not just what I learned, but how I learned it. The transition between classroom teaching, controlled practice, and real-world scenarios reinforced concepts in a truly unique, lasting way. I now feel more confident in both the medical knowledge and improvisation required to provide care in resource-limited settings.
In the hospital, it is easy to rely on systems, teams, and equipment. In the wilderness, those supports are stripped away. What remains is your ability to think, to lead, and to act with what you have.
There are a few lessons I will carry forward.
- Think in contingencies. The “Rule of Threes” applies broadly, and wilderness settings require adaptable thinking.
- Practice deliberately. These skills are rarely used day to day, and in high-stress environments like avalanche rescue or wilderness trauma management, practice allows you to perform effectively when it matters most.
- Use all available resources. This includes items carried on your patient, your environment, and using your entire team with roles established early and clearly for each member.
- Stay and play versus load and go. Prioritize what must be done immediately versus what can safely wait for definitive care.
I feel incredibly grateful to have had the opportunity to complete this elective and to have learned from such an incredible group of students and faculty. The experience reinforced my interest in wilderness medicine, but more importantly, it has given me the foundational skills and knowledge to provide care in remote settings.
As I transition into residency, I hope to carry these lessons forward, build on the skills I have learned, and contribute in some way to the growth of wilderness medicine training opportunities in Canada.