INTRODUCTION
Heat illness refers to a spectrum of diseases, ranging from minor to severe, including heat cramps, heat edema, heat syncope, heat exhaustion, and heat stroke. These conditions manifest in the setting of hyperthermia, where an individual’s core temperature exceeds its normal physiologic setpoint. While “normal” core temperatures may range between 36°C and 38°C depending on the individual, the “abnormal” threshold is typically defined as exceeding 40°C. It is important to note that being hyperthermic does not imply the presence of heat illness. Physiologic hyperthermia is a normal occurrence in exertional settings, even demonstrated in temperatures as low as 26.5°C; it is possible to have core temperatures exceeding 40°C without symptoms. While absolute temperature thresholds suggest an increased risk of heat illness, they are not, in and of themselves, purely diagnostic. Heat illness occurs when hyperthermia, due to high ambient temperatures and/or strenuous exertion, results in certain pathophysiologic processes.
The original WMS Practice Guidelines for the Treatment and Prevention of Heat-Related Illness were originally published in 2013. Since then, they were updated in 2019 and, most recently, in 2024. This article represents a summary of updates that focus on the review of classifications, pathophysiology, evidence-based guidelines for planning and preventive measures, and recommendations for field- and hospital-based therapeutic management of heat illness.
DEFINITIONS
Heat cramps, the clinical phenomenon of involuntary diffuse large muscle contractions associated with exertion in hot environments, have long been attributed to electrolyte imbalance. Heat cramps may share commonalities with exercise-associated muscle cramps (EAMC). EAMCs are known to be potentiated in heat and not clearly caused by electrolyte disturbances. The unifying hypothesis is that altered neuromuscular control is the true underlying mechanism and, therefore, may provide a better explanation for the pathophysiology of heat cramps as well.
Heat stroke is defined as a core temperature above 40°C combined with nervous system dysfunction (e.g., encephalopathy, seizures, or coma). Heat stroke must be differentiated from heat exhaustion, a mild to moderate form of heat illness that may include weakness, fatigue, thirst, headache, nausea, dizziness, and muscle aches. Heat exhaustion may progress to heat stroke if untreated, but heat stroke can occur suddenly without an identifiable phase of heat exhaustion. Heat stroke is divided into two categories: classic or non-exertional heat stroke (NEHS), caused by passive exposure to high ambient temperature, and exertional heat stroke (EHS), which results from hyperthermia during strenuous exercise.
HEAT DISSIPATION AND PATHOPHYSIOLOGY
The skin is a critical site for heat dissipation. If the skin remains at an elevated temperature due to ambient environmental conditions or clothing, it will not dissipate heat normally. This prevents normal cooling processes and results in the elevated temperature of the skin actually heating, rather than cooling, the body.
Heat stroke involves a cascade of cellular and systemic responses. The three key responses include thermoregulatory dysfunction, an acute phase response, and a heat shock protein response. The acute phase response seen in heat stroke involves inflammatory processes and reactions and is very similar to what is seen in sepsis. Prognostic scores for inflammatory response and sepsis even correlate with the fatality risk seen in heat stroke. These elevated temperatures also alter the ability of heat-shock proteins to express any cellular protection, potentially leading to end-organ dysfunction. A key point among the systemic responses and overall mortality risk is that the severity of injury, and therefore outcome, is directly related to the level and duration of thermal stress. This underscores the importance of timely treatment of patients suffering from severe heat illness.
PREVENTION AND PLANNING
Individual Factors
Multiple relatively simple recommendations can make a difference in the prevention of heat illness. Acclimatization is one of the most powerful strategies for prevention. Successive exposures to heat, even just in the course of one week, can lower physiologic strain by up to 20%. The full benefits of acclimatization are generally achieved within 10-14 days and have enduring benefits for reducing heat-related physiologic strain, even up to a month after leaving the hot environment. It is suspected that these benefits are related to increased volume expansion and sweat capacity. Suffering from heat stroke will cause a complete “reset” of thermoregulatory adaptations and increase the risk for subsequent heat injury, but over time, it is possible to recover heat tolerance.
Hydration status is another key heat illness risk factor. As little as a 2-3% decrease in body weight due to fluid losses correlates with elevated core temperatures during exertion in the heat. Dehydration further diminishes the body’s ability to cool itself effectively and increases physiologic strain and core temperatures. A “drink-to-thirst” approach, rather than a scheduled regimen, is the going recommendation for advising hydration during exertion. Doing so avoids risks associated with exercise-associated hyponatremia (EAH).
Hyperhydration using osmotic agents that augment water absorption has not been shown to be protective from heat illness, though they may decrease physiologic strain. Precooling may yield short-term exertional benefits but does not demonstrate risk reduction during longer periods of activity.
The CPG recommends screening for any significant preexisting medical condition that may increase one’s risk of heat illness. Studies show that individuals with increased body mass indices are at an increased risk of heat illness. As well as those with a history of heat injury and individuals who take medications that could limit the thermoregulatory response.
Environmental
The wet-bulb globe temperature (WBGT) index is a composite measurement of temperature, humidity, and solar radiation that expresses the total thermal strain on an individual. While WBGT is the preferred metric, it is highly localized and requires special equipment. When WBGT isn’t feasible, authors advise the use of the heat index. This is more readily available and still helps to outline heat injury risk.
FIELD TREATMENT
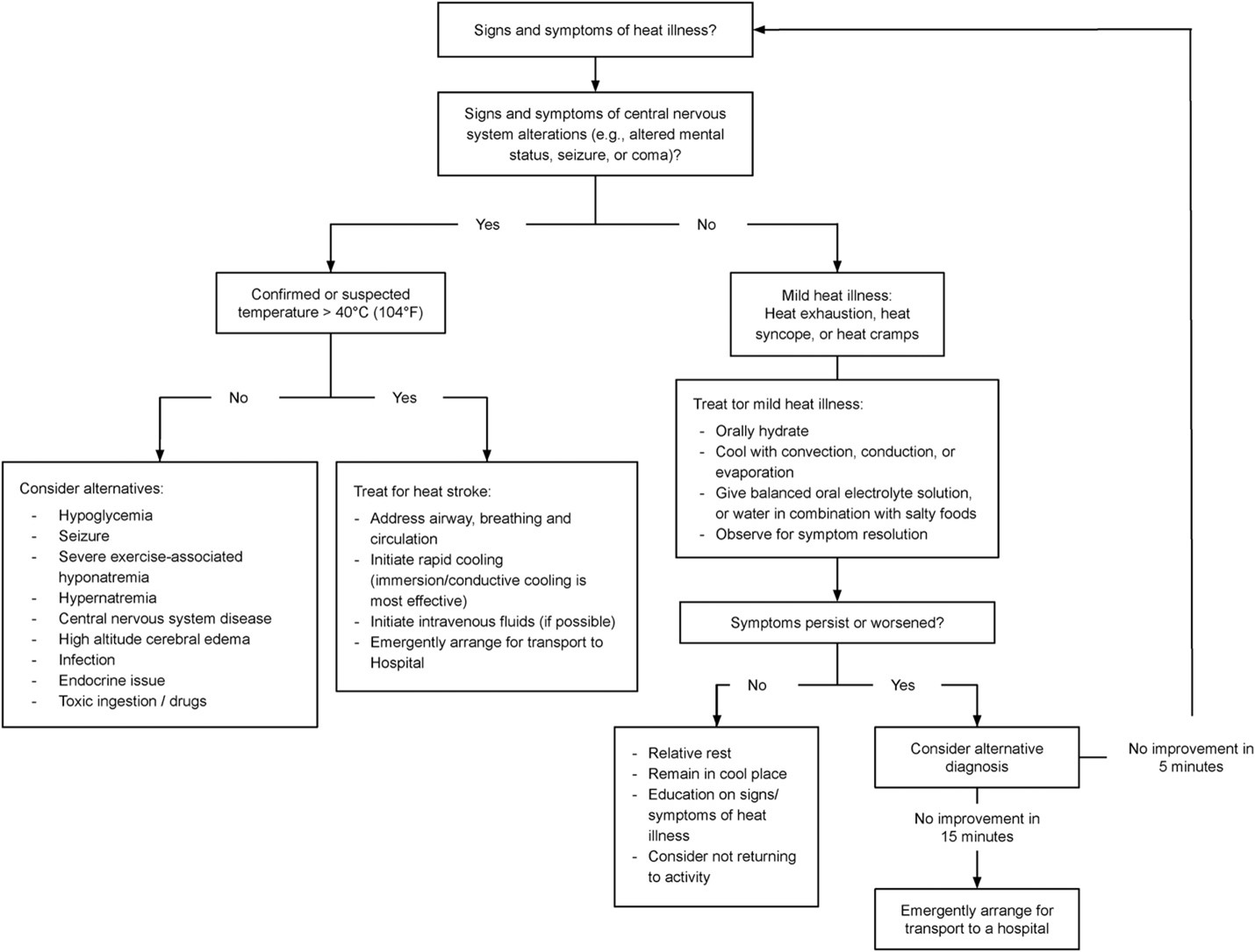
Optimal field treatment can be challenging due to resource limitations. The algorithm below demonstrates the appropriate treatment recommendations based on heat illness severity. There is one differentiation from the previous CPG update in 2019. When treating for mild heat illness, if symptoms have persisted or worsened, rather than perform more aggressive cooling measures as noted in the 2019 update, the recommendation now is to consider alternative diagnoses, and it highlights the importance of reevaluating for signs and symptoms of heat illness. Ultimately, if there is no improvement in 15 minutes, emergent transport is advised. Otherwise, the 2024 update is the same, emphasizing that cold water immersion, after appropriate airway, breathing, and circulation assessment, is the most important method of treating severe heat illness.
Temperature Measurement
Getting an accurate measurement of core temperature is important and should be performed rectally. It is important for appropriately diagnosing severe heat illness but also for excluding it and considering other forms of altered mental status when the core temperature is below 40°C. In a hyperthermic patient with altered mental status, even when core temperature is unknown, empiric active cooling is still recommended.
Hydration
Appropriate hydration levels help reduce hyperthermia, and both oral and IV hydration can be effective. In mild and moderate heat illness, oral fluid replacement is the recommended first-line therapy. IV fluids are recommended for rehydration in heat stroke, however, be mindful of the possible presence of exercise-associated hyponatremia, which may present similarly to heat exhaustion. No effort to rehydrate should delay rapid whole-body cooling.
Cold Water Immersion Therapy
Cold water immersion (CWI) therapy is the gold standard for achieving rapid temperature reduction. There is a theoretical concern that CWI could lead to peripheral vasoconstriction and shivering, which may slow the cooling process and even increase core temperatures, but military studies seem to debunk this concern. If ice water immersion is not possible, then use the coldest water available. Healthy patients who suffer exertional heat stroke (EHS) but return to baseline mental and mobility status within two hours can be released from field treatment directly to self-care without hospital transfer. Patients who experience non-exertional heat stroke (NEHS) should be transported to a higher level of care, even if they respond well to treatment. Timely use of CWI demonstrates that in some cases, patients can be effectively treated for heat stroke without the need for hospital transfer. In studies involving field treatment with CWI and subsequent observation prior to discharge, no fatalities or morbidity resulted.
Evaporative Cooling
If CWI is unavailable, evaporative cooling is the recommended second-line treatment. Remove or loosen clothing and douse the patient with cold water, ensuring that all of the skin surface area is wet. The patient then needs to be fanned. The evaporative cooling from the dousing and the convective cooling from the fanning is generally half as fast as CWI but may be easier to facilitate in a field setting.
Chemical Cold Packs and Ice Packs
A common recommendation for patient cooling has long been to put cold packs covering the neck, axillae, and groin to cool blood flowing in the major vessels and lower core temperature. Studies show no benefit in reducing heat with this technique. If ice packs are all that is available, patients should have their entire body covered. If there are not enough available, the ice packs should be placed on the cheeks, palms, and soles. A small study demonstrated that placing chemical cold packs in those areas cooled at twice the rate of traditional neck, axilla, and groin placement.
HOSPITAL TREATMENT
Ice water immersion is still considered the first-line treatment for both EHS and NEHS in the hospital setting. If this isn’t possible, then the recommendation is to cover the patient’s entire body with crushed or cubed ice. Authors recommend against the use of ice packs or icy, wet towels on the neck, axilla, and groin.
The target temperature when performing ice-water immersion is between 38.3-38.8°C. Patients cooled to this range should resume endogenous thermoregulation. Multiple studies demonstrated no fatalities or adverse outcomes when using this target temperature range.
EMERGING TRENDS
Authors currently recommend against any pharmacologic agents for the treatment of heat stroke. Dantrolene, the medication used to treat malignant hyperthermia, is currently in clinical trials for the treatment of EHS. A previous clinical trial using dantrolene in NEHS showed no improvement in cooling rates or outcomes.
Serum biomarker research is currently underway and may help predict disease severity or mortality risk in heat stroke. Currently, however, there are no conclusive recommendations on the role of biomarkers in predicting clinical outcomes or guiding the management of heat stroke.