Introduction
Eye injuries in the wilderness continue to pose a challenge for several reasons including limited access to proper equipment, medications, and specialty training for most providers. In 2024, the Wilderness Medical Society published updated guidelines on the most common eye complaints, injuries, and their respective treatments in the wilderness settings. This article summarizes those guidelines.
Pre-trip Planning and Prevention
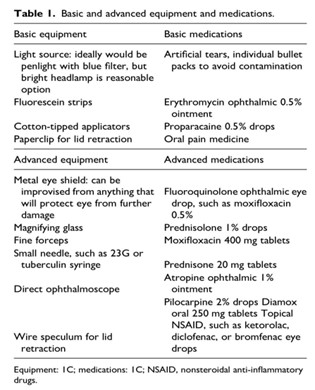
Pre-departure preparation for wilderness activities is crucial since specialized equipment and medications are often lacking. It is recommended that either a basic or advanced medical kit be brought on expeditions based on the duration, resources, and remoteness of each trip. Table (1) includes a list of eye-related equipment and medications that should be included in basic and advanced kits.
Trauma is the most common cause of eye complaints and while prevention of any injuries may be unavoidable, certain precautions can reduce these risks. Many eye afflictions can be prevented with sunglasses and other types of eye protection and good hygiene, such as proper handwashing. It is recommended that anyone with a history of ophthalmologic issues taking part in wilderness activities have a complete eye examination within three months of the trip, bring all their own eyewear and medications, a copy of their lens prescription, and extra contacts or glasses if they will be in a remote setting. The importance of proper replacement contacts and glasses cannot be overstated, as an evacuation or expedition will be infinitely more complicated for someone who cannot see properly. In particular, contact lens wearers should have backup glasses in case of an infection or other injury requiring temporary pause in contact use.
Conclusion
Eye injuries in the wilderness can be difficult to treat due to the lack of access to proper equipment and medication, as well as lack of training among providers who do not routinely treat these injuries in the urban/routine setting. Wilderness treatment for these eye complaints and injuries is thus largely based on the available equipment, medications, and need for rapid intervention and evacuation. The majority of evidence regarding wilderness treatment for eye injuries is limited to case reports and extrapolation of clinical and hospital care. With the use of proper pre-trip planning, available tools, and the knowledge of history taking and physical examination skills, the practitioner should have the ability to determine if further intervention or immediate evacuation is needed for an individual with ocular pathology.
Eye Complaints
Eye complaints can be categorized in various ways, distinguishing between traumatic and atraumatic causes, the appearance of a red or white sclera, and the presence or absence of vision loss. New-onset vision loss requires immediate evacuation.
High altitudes can pose a risk for both healthy individuals and those with a history of ocular pathology. As the cornea receives most of its oxygen from the environmental air, it can become hypoxic and lose normal function when exposed to high altitudes. Individuals with a history of intraocular bubbles should avoid travel to high altitudes due to the possibility of expansion to the bubble gas as atmospheric pressure decreases. Patients who have received radial keratotomy (RK) may experience an increase in far-sightedness and a significant decrease in visual acuity. RK patients should consult with their ophthalmologist about bringing multiple strengths of corrective lenses if recreating for prolonged periods at high altitude. Individuals who have undergone laser-assisted stromal in-situ keratomileusis (LASIK) and photo-refractive keratectomy (PRK) experience minimal to no visual changes when exposed to high altitudes.
Diving can significantly affect the eye due to increases in atmospheric pressure. Patients who have a history of surgical intraocular gas bubbles should not dive. It is safe to dive if the patient has undergone laser-assisted stromal in-situ keratomileusis (LASIK) or photo-refractive keratectomy (PRK). Those who received radial keratotomy (RK) should avoid diving for 3-6 months postoperatively. Ocular and periocular barotrauma can occur when air is compressed due to being in an enclosed space and exposed to high atmospheric pressure. This happens when the pressure inside a facemask is not equalized. This can cause severe trauma to the eye, including periorbital ecchymosis, edema, subconjunctival hemorrhage, and possibly hyphemas. Emergent evacuation is recommended if it results in a hyphema.
Ocular trauma can result in several types of injuries and is the leading cause of preventable blindness worldwide. Orbital fractures with visual changes or ocular entrapment require emergent evacuation. Retrobulbar hemorrhage, or bleeding in the orbit that can cause entrapment or elevated pressure, presents as periorbital edema, ecchymosis, diplopia, proptosis, afferent pupillary defect, or decreased extraocular motion (EOM). If there is suspicion of a retrobulbar hemorrhage causing elevated orbital pressure, a lateral cantholysis should be considered if trained personnel are available and requires emergent evacuation.
If a globe rupture is suspected, external pressure on the eye should be avoided, a covering of the eye should be placed to prevent any additional pressure or trauma, and the patient should be evacuated. If a globe rupture is suspected, penetrating foreign bodies should not be removed and splinted in place if possible. Early systemic steroid and antibiotics should be administered if available to prevent endophthalmitis. Topical antibiotics should be avoided in globe ruptures.
A hyphema is blood in the anterior chamber. This can be an isolated injury or associated with a globe rupture, dislocated lens, or retinal injury. Sequelae can include increased intraocular pressure (IOP), corneal staining, or rebleeding. In addition to emergent evacuation, activities should be restricted to walking to aid evacuation. The following medications, if available, are recommended: topical steroids, cycloplegics, tranexamic acid or aminocaproic acid, IOP-lowering medications, acetazolamide, and analgesics and antiemetics as needed. A rigid shield should be applied and nonsteroidal medications should be avoided.
Table 2: Summary of common eye complaints and injuries, noting the white-vs-red eye and traumatic vs atraumatic presentations.
|
Diagnosis
|
Category
|
Presentation
|
Cause
|
Treatment (non-wilderness)
|
Evacuation
|
|
Central Retinal Artery Occlusion (CROA)
|
White eye
|
Abrupt vision loss, painless
|
An ischemic stroke of the retina
|
-High flow oxygen
-Hyperbaric oxygen therapy
|
Emergent
|
|
Central Retinal Vein Occlusion (CRVO)
|
White eye
|
Painless vision loss, afferent pupillary defect*
|
-Thrombus
-Vasculopathy
|
-Surgical
-Topical steroid
|
Emergent
|
|
Retinal Detachment
|
White eye
|
Painless vision loss, “floaters” sensation or flashes of bright light in the visual field
|
A tear in the retina
|
Surgical
|
Emergent
|
|
Preseptal cellulitis
|
White eye
|
Swelling and inflammation of the eyelid, without involvement within the eye/orbit itself
|
Infection to the superficial tissue surrounding the eye and eyelids
|
-Antibiotics:
-Amoxicillin
-Clavulanate
-Fluoroquinolones
|
Non-emergent if it is differentiated from orbital cellulitis
|
|
Orbital cellulitis
|
White eye
|
Bulging of the eye, swelling of the conjunctiva, painful extraocular movements*, and visual disturbance
|
Infection to the soft tissue of the bony orbit
|
-Antibiotics
-Amoxicillin
-Clavulanate
-Fluoroquinolones
|
Emergent
|
|
Dacryocystitis
|
White eye
|
Pain, swelling, erythema over the lacrimal duct
|
Obstruction of the lacrimal duct
|
-Antibiotics
-Amoxicillin
-Clavulanate
-Warm compresses
|
Non-emergent
|
|
Acute angle-closure glaucoma
|
Red eye
|
-Severe pain, blurred vision, halos around lights, headache, nausea, and vomiting
-Non-reactive pupil that is mid-dilated
|
Blockage of aqueous outflow from the chamber of the eye
|
-Beta-adrenergic antagonist
-Timolol
-Carbonic anhydrase inhibitor
-Acetazolamide
-Topical
-Alpha2-adrenergic agonist
-Pilocarpine
-Patient lying flat for 1 h
-Surgical
|
Emergent
|
|
Iritis
|
Red eye
|
Pain, redness of the conjunctiva, blurred vision, and photophobia*
|
Nontraumatic inflammation of the iris
|
-Corticosteroids
-Prednisolone drops
-Oral steroids, unless there is a concern for herpetic lesions
-Prednisone
|
Emergent
|
|
Herpes Keratitis
|
Red eye
|
Inflammatory blisters or ulcers seen on a fluorescein examination
|
Ocular herpes infection
|
-Oral or ophthalmic preparations
-Trifluridine
-Acyclovir
|
Emergent
|
|
Conjunctivitis
|
Red eye
|
Pain, involves the palpebral conjunctiva*
|
Allergies, viruses, and bacteria
|
-Antibiotics
-Hand washing
-Topical anesthetic eye drops
|
Non-emergent
|
|
Periocular trauma
|
Trauma
|
Traumatic
-Eyelid lacerations (simple or complex); simple- often horizontal, partial thickness, does not include the lid margin; complex- full-thickness and involved the lid margin or medial/lateral end of the palpebral fissures
|
Trauma to the eyelid
-Fall, branches, rock, or animal bites
|
-Irrigation of the laceration
-Antibiotic ointment
-Eye shield
|
Emergent if there is a complex eyelid laceration
|
|
Orbital fractures
|
Trauma
|
Painful, possible entrapment* of ocular muscles
|
Trauma to the eye
|
-Avoid nose blowing
-Decongestant spray
-Systemic steroids
|
Emergent
|
|
Retro-orbital hemorrhage
|
Trauma
|
Painful vision loss, afferent pupillary defect, increased IOP*
|
Bleeding behind the eye
|
-Surgical
-Lateral cantholysis
|
Emergent
|
|
Globe rupture
|
Trauma
|
Painful, soft eye
|
Rupture of the structure of the eye
|
-Antibiotics
-Moxifloxacin
-Corticosteroids
-Eye shield
|
Emergent
|
|
Hyphema
|
Trauma
|
Inflammation, painful, increased IOP*
|
Trauma to the eye that causes a collection of blood between the iris and cornea
|
-Walking only
-Aminocaproic or Tranexamic acid
-Acetazolamide
-Corticosteroids or cycloplegics
-IOP-lowering medication
-Analgesics and antiemetics
-Use of a rigid shield
-Avoid NSAIDs
|
Emergent
|
|
Corneal abrasions
|
Trauma
|
-Foreign body
-Direct blow to the eye
-Use of contact lenses
-Very common
-Red eye
|
Abrasion to the cornea of the eye
|
-Topical antibiotics
-Erythromycin
-Cycloplegics
-Atropine
-NSAIDs
-Ketorolac
-Frequent use of artificial tears
-Sunglasses
-Avoid eye patching
|
Emergent if it is an open globe or deep epithelial defect
|
|
Corneal ulcers
|
Red Eye
|
-Outer eye pain, epithelial defect on fluorescein examination, white or gray infiltrate on the cornea when using penlight evaluation
-History of corneal abrasion
-Improper use of contact lens
|
Damage to the deep layers of the cornea
|
-Topical antibiotics
-Fluoroquinolone
-Oral antibiotics
Fluoroquinolones
-Cycloplegics
-Atropine drops
|
Emergent
|
|
Chemical eye injuries
|
Traumatic
|
Chemosis*, blepharitis*, corneal irritation
|
Includes but is not limited to spitting cobras, skunk musking, jellyfish stings, and exploding or spraying of cooking gasses, bear spray
|
-Large volume irrigation
-Topical antibiotics
-Oral antibiotics
|
Emergent
|
|
UV Keratitis (Snow blindness)
|
Red Eye
|
Severe pain, burning, tears
|
Inflammation of the cornea by UV rays
|
-Sunglasses with side shields
-Topical antibiotics
-Cycloplegics
-NSAIDs
-Use of artificial tears
-Avoid patching
|
Non-emergent
|
|
Traumatic iritis
|
Trauma
|
Pain, photophobia*
|
Inflammation of the anterior uveal tract after trauma occurred
|
-Topical steroids
-Prednisolone
-NSAIDs
-Cycloplegics
|
Non-emergent
|
|
Subconjunctival hemorrhage
|
Red eye, traumatic
|
Bright red spots on the eye
|
Bleeding that occurs between the conjunctiva and the sclera
|
No treatment required
|
No evacuation required
|
*Definitions:
Afferent pupillary defect: occurs when a light is shone into the normal eye, both pupils will constrict, but when the light is shone in the abnormal eye, both pupils will dilate
Blepharitis: inflammation of the eyelid
Chemosis: swelling of the conjunctiva
Entrapment: occurs when the soft tissue becomes trapped in fragments of bone and the eye cannot move in its socket
Extraocular movements: tests the muscles that are responsible for the movement of the eye
IOP: intraocular pressure of the fluid inside the globe
Palpebral conjunctiva: coats the inside of the eyelid
Photophobia: pain and sensitivity in the eye when light is shined directly into it