Activities in the outdoor and austere environments often involve exposure to bodies of water. With exposure to water sports and recreation comes the risk of drowning. In 2024, the Wilderness Medical Society published an updated version of its Practice Guidelines for the Treatment and Prevention of Drowning. These guidelines provide evidence-based recommendations to individuals and groups recreating in austere environments to 1) decrease the incidence of drowning during these activities and 2) decrease morbidity and mortality due to drowning through improved resuscitation and care.
Statistics
Drowning represents a huge disease burden, accounting for 236,000 deaths globally every year, with the highest-risk age group worldwide being children ages 1-4. The actual burden on all ages is likely underreported because most studies omit drowning deaths from storms, floods, boating, and only address fatal drownings.
Terminology
In 2002, the World Congress on Drowning established the uniform definition of drowning as “the process of experiencing respiratory impairment due to submersion or immersion in liquid.” This definition includes patients who survive the process—a conservative estimate is that for every fatal drowning, another five persons seek emergency care for non-fatal drowning. The 2002 definition has been adopted by major consensus organizations in the United States and internationally who engage in drowning prevention and treatment.
There are three outcomes from the drowning process:
- Fatal drowning
- Non-fatal drowning with injury
- Non-fatal drowning without injury
The following modifiers are no longer considered legitimate or clinically meaningful terminology and should not be used in association with drowning: near, wet, dry, active, passive, saltwater, freshwater, delayed, or secondary drowning.
Rescue of the Drowning Patient
People without formal water rescue training should only attempt rescues from a safe location by reaching with an arm or sturdy object, throwing a line or flotation device with a line, or in a safe watercraft to the drowning patient (“reaching, throwing, or rowing”). Entering the water to perform a rescue should be attempted only by persons with specific training to operate in these dangerous environments. Few studies have been conducted on the effectiveness of different water safety devices (eg, rescue tubes, rescue cans, throw bags, life rings) and some can increase risk if used incorrectly. What we do know is that proper and effective use of these devices requires basic knowledge of their function combined with regular practice. If specialized rescue equipment is available, participants should be familiar with the location and purpose of this equipment, and designated rescue personnel with proper training should use it in the event of a water rescue.
Submerged Vehicles
Drowning in vehicles is poorly understood, under-reported, and subject to much misinformation. It is critically important to escape the vehicle as quickly as possible. The mnemonic SWOC is recommended to prioritize actions: Seatbelts off, Window open, Out immediately, Children First.
In-Water Resuscitation
In-water resuscitation (IWR) is defined as the “attempt to provide ventilations to a drowning patient still in the water.” IWR should only be considered by a rescuer with adequate training and equipment to perform the skill safely and effectively. The aquatic conditions must be sufficiently safe for the rescuer to perform IWR and the point of extrication must be far enough away to justify this technically difficult task. If conditions are too hazardous to safely perform IWR, rapid extrication is indicated without a delay. Chest compressions should never be attempted in water.
CPR Priorities
Supplying oxygen to the brain is critical in drowning resuscitation. Establishing an airway and providing oxygen are the priorities in the initial resuscitation. For the patient in cardiac arrest, provide positive pressure ventilations in addition to chest compressions. Advanced airways such as intubation may be used the same as they would be for non-drowning indications.
Compression-only CPR is likely to be of little to no benefit in drowning resuscitation and its use should be limited to bystanders not trained in rescue breathing. All people whose role might involve responding to a drowning person (eg, parents, trip leaders, lifeguards) should obtain CPR training that includes both rescue breathing and chest compressions.
Oxygen
When treating a drowning patient, oxygen should be delivered at the highest concentration available. For patients in respiratory distress or not breathing, positive pressure is preferred over passive ventilation. If supplemental oxygen is not available, mouth to mouth, mouth to mask, or BVM with room air should be used.
Automated External Defibrillator (AED)
Because ventricular fibrillation (the heart rhythm addressed by defibrillators) is rare in drowning, the initial interventions for drowning of oxygenation and ventilation should not be delayed trying to get or apply an AED. Cardiac dysrhythmias can precipitate drowning in older persons and young, otherwise healthy persons, so if the AED is available, it should be used once oxygenation and ventilation have been initiated. AEDs can be used safely in wet environments and on boats, including on moving boats and boats with a metal surface like canoes.
Abdominal Thrusts
Abdominal thrusts (formerly the “Heimlich maneuver”) are not recommended at any time in the treatment of drowning patients.
Cervical Spine Precautions
Cervical spine injuries are exceedingly rare in drowning patients and typically associated with a significant mechanism. Treatment considerations for possible spinal trauma precautions should be carried out in accordance with the most current version of the Wilderness Medical Society Clinical Practice Guidelines for Spinal Cord Protection.
Cold Water Survival
Use of a USCG-approved, properly fitted life jacket that is appropriate for the conditions provides the best chance of surviving an unexpected fall into cold water. Hyperventilation caused by the cold shock response can precipitate drowning in the first one to three minutes. Upon falling into cold water, subjects should distance themselves from any immediate life threats, then remain calm and focused and control breathing by taking slow deep breaths. Then consider physical capabilities, location, resources, and chances of rescue to determine whether to swim to safety.
If a decision is made to swim to safety, this should be done as soon as possible after the cold shock response, but before physical capabilities deteriorate from the effects of cold stress.
If a decision is made to await rescue, an attempt should be made to remove as much of the body from the water as possible. All clothing should remain on, unless it hampers buoyancy. If the person remains immersed and has a flotation garment on, the heat escape lessening position should be maintained if possible. In a group, the huddle position may be used. If prolonged rescue is expected, it might be beneficial to attach oneself to a buoyant object or to a surface out of the water to improve the chance for survival.
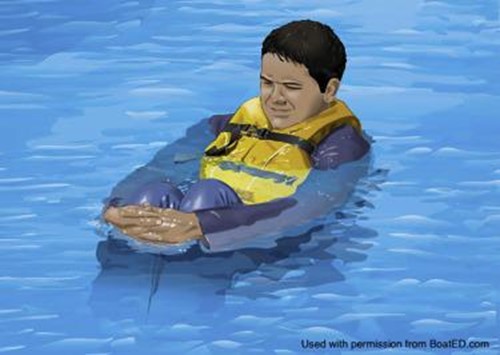
Figure 1: Heat escape lessening position (used with permission from www.Boat-Ed.com).
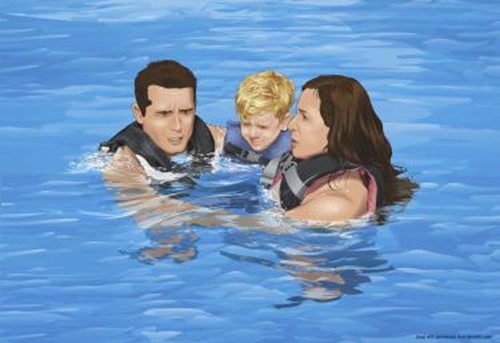
Figure 2: Huddle formation (used with permission from www.Boat-Ed.com).
Post-Resuscitation Management
Mechanical ventilation for drowning patients should follow acute respiratory distress syndrome (ARDS) protocols. Noninvasive positive pressure ventilation (NIPPV) has been used successfully in the out-of-hospital setting and may be used in alert drowning patients with mild to moderate respiratory symptoms. Caution should be taken with any patient who has altered mental status or who is actively vomiting due to concern for aspiration.
There is no evidence to support antibiotic or corticosteroid use in the out-of-hospital setting for initial treatment of drowning itself.
Although some guidelines recommend induced hypothermia in post cardiac arrest care, there is insufficient evidence to either support or discourage inducing or maintaining therapeutic hypothermia in drowning patients. The guidelines authors did note that there might be benefit to discontinuing rewarming interventions after a hypothermic drowning patient has reached the temperature range of therapeutic hypothermia, but that it has been insufficiently studied to support an evidence-based recommendation.
Disposition in the Wilderness
- Any patient with abnormal lung sounds, severe cough, frothy sputum, foamy material in the airway, depressed mentation, or hypotension warrants immediate evacuation to advanced medical care if risks of evacuation do not outweigh potential benefit.
- Any patient who is asymptomatic (other than a mild cough) and displays normal lung auscultation may be considered for release from the scene. Ideally, another individual should be with them for the next 6 hours to monitor for symptom development or the patient should be advised to seek medical assistance if symptoms develop.
- If evacuation is difficult or may compromise the overall expedition, patients with mild symptoms and normal mentation should be observed for 6 hours. Any evidence of decompensation warrants prompt evacuation if the risks of evacuation do not outweigh the potential benefit.
- If evacuation of a mildly symptomatic patient has begun and the patient becomes asymptomatic for 6 hours, canceling further evacuation and continuing previous activity may be appropriate.
Cessation of Water-Based Rescue and Resuscitation
Based on context and resources, it might be reasonable to cease rescue and resuscitation efforts when there is a known submersion time of greater than 30 minutes in water >6°C (43°F), or greater than 90 minutes in water <6°C (43°F), or after 25 minutes of continuous cardiopulmonary resuscitation.
Drowning Prevention
All patients with coronary artery disease, prolonged QT syndrome or other ion channel disorder, autism, seizure disorders, or other medical and physical impairments should be counseled about the increased risk of drowning. They should also be taught steps to mitigate the risk, such as buddy swimming and rescue devices, should they choose to participate in water activities. Given the higher rate of drowning in persons with epilepsy, they should be counseled to swim with a buddy or direct supervision.
Formal swim instruction is recommended for all children over age one. For swimming ability to serve as drowning prevention, people should have at a minimum enough experience and physical capability to maintain their head above water, tread water, and make forward progress for a distance of 25 meters (82 feet).
When boating or engaging in water sports for which lifejackets are recommended, participants should wear properly fitted life jackets that meet local regulatory specifications.
Alcohol and other intoxicating substances should be avoided before and during any water activities.